FORENSICS & BALLISTICS JFK
I will begin with some basic concepts of investigation before moving into the actual case of the JFK assassination.

Federal Rules of Evidence # 406
Habit; Routine Practice
“Evidence of the habit of a person or of the routine practice of an organization, whether corroborated or not and regardless of the presence of eyewitnesses, is relevant to prove that the conduct of the person or organization on a particular occasion was in conformity with the habit or routine practice.”
. . . . .
This rule officiates the concept of Modus Operandi as relevant evidence in criminal law.
Subsequently this rule transfers as relevant in discussion on this forum, and has to do with how the term “Fact” is used and a specific form of “information” derived from a reasonable organization of datum.
The epistemologically mature individual grasps that data points are but “beads” to be snapped together into chains in order to bring out the ‘meaning’ of datum.
In tandem with Routine Habit is the construction of the “profile” of a group or individual. That would be a catalog of the habits and routines of individuals or groups.
This can turn from an exacting science to an art form by talented individuals with long experience in such investigation and research.
Chain of Custody
Paul C. Giannelli
Case Western University School of Law, paul.giannelli@case.edu (1996)
Authentication or identification
of real evidence 1 refers to the requirement that an item of evidence be proved to be genuine, that is, that it is what its proponent claims it to be. McCormick expressed the requirement this way: “[W]hen real evidence is offered an adequate foundation for admission will require testimony first that the object offered is the object which was involved in the incident, and further that the condition of the object is substantially unchanged.”2 Federal Evidence Rule 901(a) codifies this requirement.
[…]
Police Markings
An object that is inscribed with the initials or markings of a police officer or other person may be readily identifiable. In such cases, the person converts a nonunique object into a readily identifiable one by placing distinctive markings on it. This practice, recommended in crime scene and evidence collection manuals, is well accepted in the cases. Firearms, bullets, currency, laboratory slides, and sundry other objects have been admitted into evidence, at least in part, on this basis.
[…]
Witness Uncertainty
A witness’s uncertainty in identifying an exhibit, however, affects the weight, not the admissibility, of the evidence.
(Example given here is not an applicable analog to the Parkland Bullet case)
[…]
Need for Chain of Custody
In some situations the proponent must establish a chain of custody. Such proof may be necessary either because the item of evidence is not readily identifiable, or because more than simple identification is necessary to establish the item’s relevance.
[…]
Lab Analysis
If the relevance of an exhibit depends on its subsequent laboratory analysis, identification by police markings made at the scene does not provide a sufficient foundation. The markings establish that the exhibit in court was the item seized by the police, but a chain of custody may be necessary to establish that the item seized was the item analyzed at the crime laboratory. For example, in Robinson v. Commonwealth, the court reversed a rape conviction due to a break in the chain of custody: “The mere fact that the blouse and the panties were identified (by the victim at trial] did not prove the chain of possession necessary to validate the F.B.I. analysis of them. ”
[…]
Links in Chain
The “links” in the chain of custody are those persons who have had physical custody of the object. Persons who have had access to, but not possession of, the evidence generally need not be accounted for. Such persons are not custodians. As noted by one court: “There is no rule requiring the prosecution to produce as witnesses all persons who were in a position to come into contact with the article sought to be introduced in evidence.
Failure to account for the evidence during possession by a custodian may constitute a critical break in the chain of custody. Some courts have indicated that all the links in the chain of custody must testify at triaJ.58 The prevalent view, however, is that “the fact of a ‘missing link does not prevent the admission of real evidence, so long as there is sufficient proof that the evidence is what it purports to be.
Thus, while a custodian in the chain of possession need not testify under all circumstances, the evidence should be accounted for during the time it was under that custodian’scontrol. Several recurrent examples of “missing link” cases are discussed in this article.
[…]
Burden and Standard of Proof
The burden of proving the chain of custody rests with the party offering the evidence. Prior to the adoption of the Federal Rules of Evidence, the courts described the standard of proof in various ways. The most common expression of the standard was that the offering party had to establish the identity and condition of the exhibit by a “reasonable probability.” Phrases such as “reasonable certainty” and “reasonable assurance” seem only variants of this standard. The reasonable probability standard appears to require no more than the “preponderance of evidence” or “more probable than not” standard, and some courts have explicitly expressed the standard in those terms. This standard is the typical standard in evidence law. Under this view, chain of custody “requirements go to the competency of the evidence, not merely to its credibility.” Under this view, the trial court determines whether this standard has been satisfied.
[…]
Habit Evidence
The proponent may also introduce evidence of habit or routine practice to establish the chain of custody. Federal Rule 406 provides that evidence of the routine practice of an organization is relevant to prove that the conduct of the organization “on a particular occasion was in conformity with the … routine practice.” Accordingly, evidence of the standard operating procedures of police departments and laboratories in safeguarding real evidence may be used to establish the chain of custody.
http://scholarlycommons.law.case.edu/cgi/viewcontent.cgi?article=1344&context=faculty_publications
Rule 406. Habit; Routine Practice
Evidence of a person’s habit or an organization’s routine practice may be admitted to prove that on a particular occasion the person or organization acted in accordance with the habit or routine practice. The court may admit this evidence regardless of whether it is corroborated or whether there was an eyewitness.
Notes
(Pub. L. 93–595, §1, Jan. 2, 1975, 88 Stat. 1932; Apr. 26, 2011, eff. Dec. 1, 2011.)
https://www.law.cornell.edu/rules/fre/rule_406
http://www.law.harvard.edu/publications/evidenceiii/rules/406.htm
https://en.wikipedia.org/wiki/Habit_evidence
http://apps.americanbar.org/litigation/committees/trialpractice/articles/summer2014-0914-habit-and-routine-practice-evidence.html
Crime Scene Protocol 1963
It was standard practice and mandated by FBI protocol in 1963 (up until the 1980s) to mark a shell or hull with a unique mark for chains of custody.
“Police Markings”
See:
Federal Bureau of Investigation, Handbook of Forensic Science 100 (rev. ed. 1984); C. O’Hara
************************************************************************************
Crime Scene Investigation
http://www.nmsoh.org/homicide_investigator_checklist.htm
https://forensicsciences.columbian.gwu.edu/master-science-crime-scene-investigation
http://science.howstuffworks.com/bloodstain-pattern-analysis.htm
************************************************************************************
Autopsy Protocol
http://www.forensicpathologyonline.com/e-book/autopsy
https://i1.wp.com/healthfavo.com/wp-
FORENSIC AUTOPSY PERFORMANCE STANDARDS
The National Association of Medical Examiners
Standard F22 Neck
The muscles, soft tissues, airways, and vascular structures of the anterior neck must be examined to identify signs of disease, injury, and therapy. A layer-by-layer dissection is necessary for proper evaluation of trauma to the anterior neck. Removal and ex situ dissection of the upper airway, pharynx, and upper esophagus is a necessary component of this evaluation. A dissection of the posterior neck is necessary when occult neck injury is suspected. The forensic pathologist shall:
F22.1 examine in situ muscles and soft tissues of the anterior neck.
F22.2 ensure proper removal of neck organs and airways.
F22.3 examine neck organs and airways.
F22.4 dissect the posterior neck in cases of suspected occult neck injury.
F22.5 perform anterior neck dissection in neck trauma cases.
Standard F23 Penetrating Injuries, Including Gunshot and Sharp Force Injuries
Documentation of penetrating injuries as listed below should include detail sufficient to provide meaningful information to users of the forensic autopsy report, and to permit another forensic pathologist to draw independent conclusions based on the documentation. The recovery and documentation of foreign bodies is important for evidentiary purposes. Internal wound pathway(s) shall be described according to organs and tissues and size of defects of these organs and tissues. The forensic pathologist shall:
F23.1 correlate internal injury to external injury
F23.2 describe and document the track of wound
F23.3 describe and document the direction of wound
F23.4 recover foreign bodies of evidentiary value
F23.5 describe and document recovered foreign body
Standard G30 Evidence Processing
Custodial maintenance and chain of custody are legally required elements for documenting the handling of
evidence. The forensic pathologist or representative shall:
G30.1 collect, package, label, and preserve all evidentiary items.
G30.2 document chain of custody of all evidentiary items
\\][//
************************************************************************************
content/uploads/2013/08/annotatedhumanskullanatomysideviewbyshevans-dglgl.png
. . .
The deposition of DR. JAMES JOSEPH HUMES BEFORE THE ASSASSINATION RECORDS REVIEW BOARD
Re: PRESIDENT JOHN F. KENNEDYCollege Park, Maryland on Tuesday, February 13, 1996
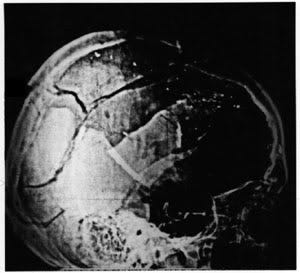
Q. Could you describe how the President’s head looked at the very first time that you saw it after it had been unwrapped?
A. Well, the most obvious thing was a large defect in the right parietal area. The
measurements are in the autopsy protocol, and the hair was matted in that area and bloody and so forth. And there was a suggestion like a contusion in the right frontal area over the right eyebrow. The skin was a little bit discolored in that area, but it wasn’t very remarkable. The most striking thing was this large defect. His face was, for all intents and purposes, normal. Normal as anybody can be in death, I guess. It was not significantly injured in any way.Q. Were any portions of the brain extruding from any wounds in the head?
A. Well, the wound was so big that–I don’t know what you mean by extruding. It wasn’t really- -it was just a gaping hole and the brain was right there. It wasn’t really being extruded, no.
Q. So you could see it, but it was not as if it were coming out–
A. No.
Q. –sort of just seeing inside a hole–
A. It was a big hole, yeah.
[…]
Q. Right below the middle of the skull, there is the number 17 with, again, arrows pointing, at least on the paper, up and down. Do you see that?
A. Yeah. I would presume that this is the antero-posterior maximum measurement of this defect. Okay?Q. Okay.
A. So it was 17 centimeters (approx 6.7 in), fore and aft, if you will, and 10 wide (4 in). I got some slightly different measurement, I think, in my written report, but ball park, you know.
Q. Right below the 17 and the arrow, there’s the word, it looks as if it’s “missing.” Do you see that?
A. That much bone is missing. That was a big defect, you see.
Q. Now, when this 10 by 17 centimeters of bone is missing, does that mean that it was present nowhere in the autopsy room during the autopsy?
A. Not until later when part of it was brought to me, which I described, I believe, in the written report.Q. So would it–
A. The pieces that were brought to me, it was either two or three, I think three: one pretty sizable one and two smaller ones. Again, I’m talking off the top of my head. When they were repositioned to where they should have been, there was still a defect. We didn’t have sufficient bone to totally close the defect.
Q. So then from the first time that you saw the President’s head without the pieces of skull fragment that came in later, the approximate measurements of the missing scalp would be roughly 10 centimeters to 17 centimeters?
A. By 17, right.
Q. In the autopsy protocol, you referred to the amount as being 10 centimeters by 13 centimeters, and let me show you the protocol.
A. I’m not going to debate it. I mean, it would depend on how you were measuring it, because it wasn’t a–like this room is 25 by 35. It’s got walls and extreme–this was irregular, so you could make any kind of measurement you want…
[…]
Q. Was scalp missing from that same–from those same measurements?A. Not as much scalp. There was some scalp missing, but we were able to pretty much close the scalp, skin, when we finished everything. So I can’t tell you how much was–but it was not that much skin missing, no.
Q. So mostly skull fragments–
A. Right.
Q. –but not the scalp itself?
A. Right. Right.
[…]
Q. The next question I wanted to ask you would be where, as best you recall, the lacerations were on just the scalp.A. They went in every direction. They were– I think I described them as stellate. So they went down this way and back, and the whole area was lacerated.
Q. For the scalp?
A. Yes.
Q. In towards the back of the head, so in the occipital–
A. Not really. Not really. The parietal region primarily. Parietal and to some extent occipital, but primarily parietal.
Q. Okay. Just for any scalp lacerations, were there any tears over the occipital bone?
A. No. No.
Q. None whatsoever?
A. No.
Q. There were tears, however, over the temporal–
A. Temporal and parietal
.
Q. And the parietal.A. Yes.
[…]
Q. Do you have any recollection now about radio-opaque objects being in or appearing in the X-rays?A. Yes, in the skull. There were some little tiny fragments of radio-opaque material, which we thought to be bullet fragments, traversing from– well, I don’t know. It looked like it was going from posterior to anterior. Very fine, sort of granular-looking material, went almost as far forward as the frontal bone, but not quite that far.
Q. Those are dust-like fragments?
A. Yes, right.
Q. Were there any–
A. A couple of them were–we did retrieve a couple that were maybe a couple millimeters, as I recall, from that path, you know. But that was about all.
Q. Do you recall where you retrieved those fragments?A. I think from the frontal lobe of the brain.
Q. Were there any X-rays taken between the time that you–or after the time that you removed the small fragments?
A. No.
Q. So all of the X-rays of the cranium were taken before any–
A. Exactly.
Q. –metal fragments were removed?
A. Exactly, exactly.
Q. Do you have any recollection now about the shapes of the fragments that were removed?
A. They were small and irregular. That’s all I can tell you.
Q. Long and sliver-like or roundish or–any recollection?
A. Flat, irregular, two or three millimeters.
[…]
Q. Dr. Humes, let me show you part of your testimony to the HSCA. Question by Mr. Cornwell– I’ll read this into the record. It’s from page 330, and it is Exhibit 21 to this deposition.
“Mr. Cornwell: And you finally began to write the autopsy report at what time?”
“Dr. Humes: It was decided that three people couldn’t write the report simultaneously, so I assumed the responsibility for writing the report, which I began about 11 o’clock in the evening of Saturday November 23rd, having wrestled with it for four or five, six hours in the afternoon, and worked on it until 3 or 4 o’clock in the morning of Sunday, the 24th.”“Mr. Cornwell: Did you have any notes or records at that point as to the exact location of the –
“Dr. Humes: I had the draft notes which we had prepared in the autopsy room, which I copied.”
Now, again, the question would be: Did you copy the notes so that you would have a version of the notes without the blood on them but still notes rather than a draft report?
A. Yes, precisely. Yes. And from that I made a first draft, and then I destroyed the first draft and the notes.
Q. So there were, then, two sorts of documents that were burned: one, the draft notes, and, two, a draft report?
A. Right.
Q. Is that correct?
A. That’s right. So that the only thing remaining was the one that you have.
Q. Why did you burn the draft report as opposed to the draft notes?
A. I don’t recall. I don’t know. There was no reason–see, we’re splitting hairs here, and I’ll tell you, it’s getting to me a little bit, as you may be able to detect. The only thing I wanted to finish to hand over to whomever, in this case Admiral Burkley, was my completed version. So I burned everything else. Now, why I didn’t burn the thing that J wrote, I have no way of knowing. But whether it was a draft or whether it was the notes or what, I don’t know. There was nothing left when I got finished with it, in any event, but the thing that you now have, period.
Q. Well, the concern, of course, is if there is a record related to the autopsy that is destroyed, we’re interested in finding out what the exact circumstances–
A. I’ve told you what the circumstances were. I used it only as an aide-memoire to do what I was doing and then destroyed it. Is that hard to understand?
Q. When I first asked the question, you explained that the reason that you had destroyed it was that it had the blood of the President on it.
A. Right.
Q. The draft report, of course, would not have had the blood of–
A. Well, it may have had errors in spelling or I don’t know what was the matter with it, or whether I even ever did that. I don’t know. I can’t recall. I absolutely can’t recall, and I apologize for that. But that’s the way the cookie crumbles. I didn’t want anything to remain that some squirrel would grab on and make whatever use that they might. Now, whether you felt that was reasonable or not, I don’t know. But it doesn’t make any difference because that was my decision and mine alone. Nobody else’s.
[…]
Q. You’re welcome to read as much as you would prefer.A. Whatever.
Q. It’s just I have a question for you on the first sentence only.
A. Okay.Q. You see that Dr. Burkley identifies the posterior back at about the level of the third thoracic vertebra. Do you see that?
A. Yes.
Q. Was that correct?
A. I don’t know. I didn’t measure from which vertebra it was. It’s sometimes hard to decide which vertebra, to tell you the truth, by palpation. Maybe you can do it accurately because the first and second–did I say the third? Oh, he says third thoracic. I think that’s much lower than it actually was. I think it’s much lower than it actually–you have seven cervical vertebrae. I don’t know. I mean, he’s got a right to say anything he wants, but I never saw it before, and I don’t have an opinion about it.
Q. Did you ever discuss which vertebra–
A. I never discussed anything about it with George Burkley, period, or anybody else.
I mean, with all due respect, you seem to have come to me from left field. You know, I just- -they’re not things of which I’m aware.
The measurements I made, as far as I’m concerned, were accurate. You could debate whether they were wise choices to be made or not, but they were accurate.
http://jfkassassination.net/russ/testimony/humesa.htm
. . .It is my opinion that from the moment JFK’s body was removed from Parkland Hospital, a medical cover-up was assured.
The so-called “autopsy” at Bethesda was beyond incompetent, it was criminal negligence__a complete fraud. This can only indicate one thing: CONSPIRACY.
ROBERT McCLELLAND, MD: In testimony at Parkland taken before Arlen Specter on 3-21-64, McClelland described the head wound as, “…I could very closely examine the head wound, and I noted that the right posterior portion of the skull had been extremely blasted. It had been shattered…so that the parietal bone was protruded up through the scalp and seemed to be fractured almost along its right posterior half, as well as some of the occipital bone being fractured in its lateral half, and this sprung open the bones that I mentioned in such a way that you could actually look down into the skull cavity itself and see that probably a third or so, at least, of the brain tissue, posterior cerebral tissue and some of the cerebellar tissue had been blasted out….” (WC–V6:33) Later he said, “…unfortunately the loss of blood and the loss of cerebral and cerebellar tissues were so great that the efforts (to save Kennedy’s life) were of no avail.” (Emphasis added throughout) (WC–V6:34) McClelland made clear that he thought the rear wound in the skull was an exit wound (WC-V6:35,37). McClelland ascribed the cause of death to, “…massive head injuries with loss of large amounts of cerebral and cerebellar tissues and massive blood loss.” (WC–V6:34)
McClelland’s unwillingness to change his recollection has recently attracted detractors in the aftermath of Charles Crenshaw’s book, “Conspiracy of Silence”. McClelland told Posner, “I saw a piece of cerebellum fall out on the stretcher.” (Posner, G. “CC.”, p. 311, paper). To dismiss McClelland, Posner quotes Malcolm Perry, “I am astonished that Bob (McClelland) would say that… It shows such poor judgment, and usually he has such good judgment.” (Posner G. “Case Closed”. p. 311, paperback edition.) Perry’s own inconsistent and unreliable memory lessens the merit of his opinions of others, as we will see.
3) MARION THOMAS JENKINS, MD: In a contemporaneous note dated 11-22-63, Jenkins described “a great laceration on the right side of the head (temporal and occipital) (sic), causing a great defect in the skull plate so that there was herniation and laceration of great areas of the brain, even to the extent that the cerebellum had protruded from the wound.” (WC–Exhibit #392) To the Warren Commission’s Arlen Specter Dr. Jenkins said, “Part of the brain was herniated. I really think part of the cerebellum, as I recognized it, was herniated from the wound…” (WC–V6:48) Jenkins told Specter that the temporal and occipital wound was a wound of exit, “…the wound with the exploded area of the scalp, as I interpreted it being exploded, I would interpret it being a wound of exit…” (WC–V6:51.)
Jenkins described a wound in JFK’s left temple to Specter. Jenkins: “…I thought there was a wound on the left temporal area, right in the hairline and right above the zygomatic process.” Specter: “The autopsy report discloses no such development, Dr. Jenkins.” Jenkins: “Well, I was feeling for–I was palpating here for a pulse to see whether the closed chest cardiac massage was effective or not and this probably was some blood that had come from the other point and so I thought there was a wound there also.” A few moments later Jenkins again pursued the possibility that there had been a wound in the left temple: “…I asked you a little bit ago if there was a wound in the left temporal area, right above the zygomatic bone in the hairline, because there was blood there and I thought there might have been a wound there (indicating) (sic). Specter: “Indicating the left temporal area?” Jenkins: “Yes; the left temporal, which could have been a point of entrance and exit here (indicating) (sic-presumably pointing to where he had identified the wound in prior testimony–the right rear of the skull), but you have answered that for me (that ‘the autopsy report discloses no such development’).” (WC-V6:51)
In an interview with the HSCA’s Andy Purdy on 11-10-77 Marion Jenkins was said to have expressed that as an anesthesiologist he (Jenkins) “…was positioned at the head of the table so he had one of the closest views of the head wound…believes he was ‘…the only one who knew the extent of the head wound.’) (sic)…Regarding the head wound, Dr. Jenkins said that only one segment of bone was blown out–it was a segment of occipital or temporal bone. He noted that a portion of the cerebellum (lower rear brain) (sic) was hanging out from a hole in the right–rear of the head.” (Emphasis added) (HSCA-V7:286-287) In an interview with the American Medical News published on 11-24-78 Jenkins said, “…(Kennedy) had part of his head blown away and part of his cerebellum was hanging out.”.
CHARLES JAMES CARRICO, MD: On the day of the assassination he hand wrote, ” (the skull) wound had avulsed the calvarium and shredded brain tissue present with profuse oozing… attempts to control slow oozing from cerebral and cerebellar tissue via packs instituted…” (CE 392–WC V17:4-5)
In is first mention of JFK’s skull wound to the Warren Commission on 3/25/64, Carrico said, “There seemed to be a 4 to 5 cm. area of avulsion of the scalp and the skull was fragmented and bleeding cerebral and cerebellar tissue.” (6H3) And… “The (skull) wound that I saw was a large gaping wound, located in the right occipitoparietal area. I would estimate to be about 5 to 7 cm. in size, more or less circular, with avulsions of the calvarium and scalp tissue. As I stated before, I believe there was shredded macerated cerebral and cerebellar tissues both in the wounds and on the fragments of the skull attached to the dura.” (6H6)
On 3/30/64 Carrico appeared again before the Commission. Arlen Specter asked, “Will you describe as specifically as you can the head wound which you have already mentioned briefly?” Dr. Carrico: “Sure. This was a 5 by 71 cm (sic–the author feels certain that Dr. Carrico must have said “5 by 7 cm) defect in the posterior skull, the occipital region. There was an absence of the calvarium or skull in this area, with shredded tissue, brain tissue present…”. Specter: “Was any other wound observed on the head in addition to this large opening where the skull was absent?” Carrico: “No other wound on the head.”(WC–V3:361)
In an interview with Andy Purdy for the HSCA on 1-11-78, Dr. Carrico said, “The skull wound” …was a fairly large wound in the right side of the head, in the parietal, occipital area. (sic) One could see blood and brains, both cerebellum and cerebrum fragments in that wound.” (sic) (HSCA-V7:268)
MALCOLM PERRY, MD: In a note written at Parkland Hospital and dated, 11-22-63 Dr., Perry described the head wound as, “A large wound of the right posterior cranium…” (WC–V17:6–CE#392) Describing Kennedy’s appearance to the Warren Commission’s Arlen Specter Dr. Perry stated, “Yes, there was a large avulsive wound on the right posterior cranium….” (WC- V3:368) Later to Specter: “…I noted a large avulsive wound of the right parietal occipital area, in which both scalp and portions of skull were absent, and there was severe laceration of underlying brain tissue…” (WC–V3:372) In an interview with the HSCA’s Andy Purdy in 1-11-78 Mr. Purdy reported that “Dr. Perry… believed the head wound was located on the “occipital parietal” (sic) region of the skull and that the right posterior aspect of the skull was missing…” (HSCA- V7:292-293) Perry told Mr. Purdy: “I looked at the head wound briefly by leaning over the table and noticed that the parietal occipital head wound was largely avulsive and there was visible brain tissue in the macard and some cerebellum seen…” (HSCA-V7:302-interview with Purdy 1-11-78.
RONALD COY JONES: was a senior General Surgery resident physician at Parkland Hospital. Under oath he told the Warren Commission’s Arlen Specter, “…he had a large wound in the right posterior side of the head… There was large defect in the back side of the head as the President lay on the cart with what appeared to be some brain hanging out of this wound with multiple pieces of skull noted next with the brain and with a tremendous amount of clot and blood.” (WC-V6:53-54) A few minutes later he described “what appeared to be an exit wound in the posterior portion of the skull”. (Emphasis added throughout) (WC-V6:56)
GENE AIKIN, MD: an anesthesiologist at Parkland told the Warren Commission under oath, “The back of the right occipital
parietal portion of his head was shattered with brain substance extruding.” (WC-V6:65.) He later opined, “I assume the right occipital parietal region was the exit, so to speak, that he had probably been hit on the other side of the head, or at least tangentially in the back of the head…”. (WC-V6:67)PAUL PETERS, MD: a resident physician at Parkland described the head wound to the Warren Commission’s Arlen Specter under oath as, “…I noticed that there was a large defect in the occiput…It seemed to me that in the right occipital parietal area that there was a large defect.” (WC-V6:71)
CHARLES CRENSHAW, MD: a resident physician at Parkland neither wrote his observations contemporaneously or was interviewed by the Warren Commission. He, with co-authors, Jess Hansen and Gary Shaw, recently published a book, JFK: Conspiracy of Silence, ” (Crenshaw, CA, Hansen, J, Shaw, G. ( JFK: Conspiracy of Silence, 1992, New York, Signet). Crenshaw has claimed both in his book and in public interviews that the President’s head wound was posterior on the right side. In JFK: Conspiracy of Silence, he wrote, “I walked to the President’s head to get a closer look. His entire right cerebral hemisphere appeared to be gone. It looked like a crater–an empty cavity. All I could see there was mangled, bloody tissue. From the damage I saw, there was no doubt in my mind that the bullet had entered his head through the front, and as it surgically passed through his cranium, the missile obliterated part of the temporal and all the parietal and occipital lobes before it lacerated the cerebellum.” ( JFK: Conspiracy of Silence, p. 86)
CHARLES RUFUS BAXTER, MD: a resident physician at Parkland in a hand written note prepared on 11-22-63 and published in the Warren Report (p. 523) Baxter wrote, “…the right temporal and occipital bones were missing (emphasis added) and the brain was lying on the table…” (WR:523). Very oddly, as Wallace Milam pointed out to one of the authors (Aguilar), when asked to read his own hand written report into the record before the Warren Commission’s Arlen Specter the words are recorded exactly as he wrote them, except for the above sentence. That sentence was recorded by the Warren Commission and reads “…the right temporal and parietal bones were missing. (emphasis added)…”. (WC-V6:44) It is reasonable to assume that Baxter’s original description of a more rearward wound is more reliable than his later testimony before Arlen Specter, who on more than one occasion tried to move the skull wound away from the rear. Baxter then described the head wound saying, “…literally the right side of his head had been blown off. With this and the observation that the cerebellum was present….” (WC-V6:41) Thus the wound he saw was more likely to have been “temporo-occipital” than “temporo-parietal”, because he also recalled, “cerebellum was present”. (WC-V6:41) Shortly later in the same interview he also said, “…the temporal and parietal bones were missing and the brain was lying on the table….” (WC-V6:44) The authors are unaware of any explanation for the discrepancies, and can only speculate that either Baxter was misquoted twice or he adjusted his testimony to conform with what he might have felt was wanted of him. The mystery was confounded when author Livingstone reported that Baxter described the skull wound as “…a large gaping wound in the occipital area.” Livingstone also reported that “(Baxter) could not have been more clear when he rejected the official picture (showing the rear scalp intact).”(Groden & Livingstone, High Treason, 1989, New York, Berkley Books, p. 45)
PAT HUTTON, RN: a nurse at Parkland who met the limousine and helped to wheel the President into Trauma Room 1 wrote a report soon after claiming, “Mr. Kennedy was bleeding profusely from a wound in the back of his head, and was lying there unresponsive.” (Price Exhibit V21 H 216–Emphasis added). While helping with resuscitation efforts a physician asked her to apply a pressure dressing to the head wound, she observed, however, that, “This was no use, however, because of the massive opening in the back of the head.” (IBID)
DORIS NELSON, RN: was a supervising nurse at Parkland. She was interviewed by Arlen Specter for the Warren Commission and she was neither asked or volunteered information regarding the nature of JFK’s wounds. (WC-V6:143-147) As Groden and Livingstone reported, however, journalist Ben Bradlee, Jr. asked her, “Did you get a good look at his head injuries?” Nelson: “A very good look…When we wrapped him up and put him in the coffin. I saw his whole head.” Asked about the accuracy of the HSCA autopsy photographs she reacted: “No. It’s not true. Because there was no hair back there. There wasn’t even hair back there. It was blown away. Some of his head was blown away and his brains were fallen down on the stretcher.” (High Treason I. p. 454)
SECRET SERVICE AGENT WILLIAM GREER: described the President’s wounds upon arrival at Parkland to Arlen Specter of the Warren Commission: “His head was all shot, this whole part was all a matter of blood like he had been hit.” Specter, “Indicating the top and right rear side of the head?” Greer: “Yes, sir; it looked like that was all blown off.”(WCV2:124)
SECRET SERVICE AGENT CLINT HILL: described the wounds he saw at Parkland as, “The right rear portion of his head was missing. It was lying in the rear seat of the car. His brain was exposed…There was so much blood you could not tell if there had been any other wound or not, except for the one large gaping wound in the right rear portion of the head.” (WC–V2:141)
http://www.assassinationweb.com/ag6.htmThe Criteria for Assessing the Reliability of Witness Testimony
The most critical would be:
1. — POV — and Distance from event witnessed
2. –- Consideration of obstructions a witness’ position would encounter
3. –- Human perception of events that occur in a matter of seconds and less
4. — The likelihood of a duck response to a nearby dangerous event.
5. — Possible conflict of interests
6. — Obvious conflict of interests
7. — Internal conflicts of a single witness’ testimony, and a detailed analysis of how this might be understood. (see 3rd criteria point)
8. — MO; Established history of lying
9. — Conflicts with known and established empirical evidence.
10. — Particular circumstances of specific witnesses, that could effect the reliability of a certain witness (Handicaps, etc).
___________________________________________________________________________________________
“The measurements I made, as far as I’m concerned, were accurate. You could debate whether they were wise choices to be made or not, but they were accurate.”~Dr Humes – testimony before ARRB
This witness testimony touches on Points 6,7,8,9,&10. One need not debate whether the choices were wise, they were clearly not – it is absurd; it is senseless when there are fixed anatomical landmarks nearby. Humes chose to measure the position of JFK’s back wound from the Mastoid Process to the Acromion – a distance that can very 70% depending on the relative positions of the head and shoulder; thus it is a rather preposterous choice for such a measurement. Thus, the measurement is inaccurate by lack of proper criteria.Furthermore; The location given by Humes conflicts with known and established empirical evidence [#9]
There is an established history of Humes lying about the notes and number of autopsy reports [#8]
There is evidence that Humes initially did place the back wound at T3 in earlier notes and reports [#7]
Humes has a ‘conflict of interest’ as he is a participant in a cover-up [#6]JOHN F. KENNEDY’S FATAL WOUNDS: THE WITNESSES AND THE INTERPRETATIONS FROM 1963 TO THE PRESENT
by, Gary L. Aguilar, MD
San Francisco, California, August, 1994“That JFK’s head wound was on the right side of his head is universally accepted. With a single exception, all witnesses placed JFK’s major skull defect on the right side, and given the frequency of witness error, this suggests good witness reliability in this case. The most peculiar aspect of JFK’s wounds is that of the 46 witnesses whose opinions I have examined between Parkland and Bethesda, 45 of whom correctly claimed that the skull defect was on the right side, 44 were apparently wrong by the “best” evidence to claim that the wound was in the right-rear, rather than the right-front. The “authenticated” photographs, the originals of which were twice examined by author Aguilar at the National Archives, show no rear defect at all, only an anterior-lateral defect, and so, if valid, the images prove that not a single witness accurately described JFK’s fatal wound, and that even the autopsy report fails to accurately describe the skull defect visible in the images!
The HSCA’s forensic panel, which delved into the mysteries of JFK’s autopsy, accepted the authenticity of the current inventory of X-rays and photographs. Principally on the basis of these images, the panel concluded that the autopsists missed the correct location for the entrance bullet wound to the skull by placing it 10-cm too low, and missed the location of the bullet entrance to JFK’s back by placing it 5-cm too high. While the HSCA’s forensic panel apparently never considered the overwhelming witness testimony that there was a rear defect in JFK’s scalp/skull, it follows that all the witnesses were wrong if the images are right. To add to the muddle, recently revealed documents cast doubt on at least the completeness of the photographic inventory, and the technicians who took JFK’s X-rays and photographs both insist the current images are not those they took.”
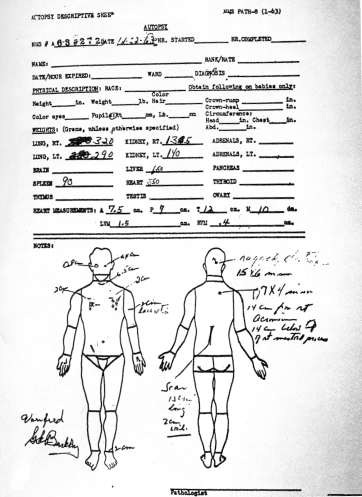
Dr Boswell’s Face Sheet
9.2.4 Special Wound Ballistics of the Head
In intracranial gunshot wounds, several of the above-mentioned factors enhance the degree of tissue disruption. The inelastic quality and the high water content of brain tissue make it per se very vulnerable to cavitation and stretch-mechanism. The penetration of the skull can imply the generation of secondary missiles in the form of bone (Fig. 9.7) or bullet fragments [28, 41, 42, 43, 44] and a tendency towards early tumbling or deformation of the bullet. Kirkpatrick and DiMaio [44], for example, were able to demonstrate intracerebral bone chips solely by digital palpation of the brain in 16 out of 42 cases of civilian gunshot wounds to the brain. Even more important, intracranial trajectories gain a new quality by the rigid skull functioning as a non-yielding wall. Because brain tissue is almost incompressible, intracranial temporary cavitation and surrounding overpressure meet counter-pressure from the skull.
The skull will, so to speak, try to overcome the principle of nonconfinement of the cavity by denying the free space necessary for a gradual decrease of radial tissue displacement and associated overpressure. The volume of the intracranial temporary cavity will consequently stay smaller than a cavity formed under identical conditions in tissue not confined in a casing. Intracranial overpressures around the expanding temporary cavity, however, clearly exceed the pressures found in nonconfined tissue [4, 10, 45, 46]. These high dynamic pressures, the asymmetric shape of the temporary cavity, and unilaterally fixed tissue structures lead to shear forces within brain tissue. The unyielding skull does not allow the brain to expand, so the brain will transfer the overpressures to the skull. In other words, the brain’s surface gets pushed with great force against the inner table of the neurocranium and the brain stem gets forced down into the foramen magnum.
Consequently, the layer of cerebral tissue between temporary cavity and skull is compressed much more strongly than tissue not confined in a rigid casing and shearing of brain tissue is increased by bone structures projecting into the skull cavity. Analogous to blunt trauma, enhanced compression can result in contusion of brain tissue discernible as (cortical) contusion zones in superficial layers of the brain remote from the trajectory [28, 44, 47, 48, 49] (Fig. 9.8). The stretching and especially shearing of tissue is responsible for intracerebral petechial hemorrhages remote from the tract in the form of classical perivascular ring hemorrhages or spherical hemorrhages [28, 41, 43] (Fig. 9.9). They are simply the result of an enlarged zone of extravasation due to the enhanced effect of temporary cavitation.
Preferential neuroanatomical sites are more central parts of the brain such as the basal ganglia, midbrain, pons, and cerebellum The skull will at first be slightly stretched by intracranial overpressures. If the skull’s capacity to elastically stretch is surpassed, there will be indirect skull fractures, i.e., fracture lines without contact to the primary bony entrance and exit defects. Because the base of the skull is inhomogenous and less resistant to stretching than the vault, preferential locations are the roofs of the orbitae (Fig. 9.10) and the ethmoidal plates in the anterior cranial fossa [50]. While secondary radial fractures originating from the gunshot defects are induced by the bullet’s impact, tertiary concentric fractures connecting the radial fracture lines (Fig. 9.11) are indirect heaving fractures [51, 52, 53] functioning as additional stress relief for internal overpressures. If the internal pressures are high enough, indirect skull fractures will combine to an ‘‘explosive’’ type of head injury [54] with comminuted fractures of the skull and laceration of the brain.
____________________________________________________________________________________
Sherry Fiester – CSIInvestigation into the bllistics of the JFK assassination

PHOTOGRAMMETRY
The illustration above is the product of photogrammetry Photogrammetry is the science of making measurements from photographs, especially for recovering the exact positions of surface points. Moreover, it may be used to recover the motion pathways of designated reference point – Illistration by Sherry Fiestern the years since President Kennedy’s death, various technical fields have made great strides in understanding ballistics. Developing accurate methods to establish projectile trajectories and establishing a better understanding of wound ballistics continues to be the focus of new research and technical publications. Scientifically establishing directionality of the projectile striking Kennedy in the head is paramount TO EITHER support a single rear shooter, OR establishing a conspiracy. Beveling, fracture sequencing, and projectile fragmentation, target movement, and blood spatter in gunshot wounds to the head are current methods of assessing a projectile’s direction of travel. Application of the latest forensic technology and research provides new pieces of the assassination puzzle. Identifying the head shot as a front or rear injury is significant as it proves a conspiracy to assassinate President Kennedy. Contemporary research indicates of the five methods to determine the direction of travel of the projectile fatally wounding President Kennedy. One is deemed unreliable, and the other four support a shot from the front. Importantly, they do so while meeting the evidentiary standard required to support a criminal conviction in today’s courtroom.
Beveling
Bullets traveling through bone create marginal conical shaped fractures adjacent to the entry or exit site. The conical beveling characteristically appears as a symmetrical chipping out of bone forming an indentation surrounding the entry or exit point on the opposite side of impact. The small end of the cone touches the interior or exterior bone table from which the bullet entered. Tangential gunshot wounds to the head create elliptically shaped defects containing both internal and external beveling (Levy, 2012).
Some wounds present both internal and external beveling. Researchers attribute this pseudo-beveling in high velocity distance shots to the transference of kinetic energy to the skull as dislodged chips flaking off entry wound edges, producing the effect of beveling. Without careful examination, misinterpretation of an entrance wound as an exit wound is possible in all types of entries (Quatrehomme, 1998, Coe, 1981; Prahlow, 2010; Adams, 2010).
Based upon current forensic research, it appears beveling cannot provide conclusive evidence of projectile direction. Incorrect assessment of direction can occur with tangential entries or exits, mistaken orientation, insufficient beveling, or the failure to recognize external beveling on entry wounds.
Fracture Patterns
When a projectile strikes the skull, radial fractures are created which extend outward from the wound. Internal pressure from temporary cavitation produces concentric fractures create that are perpendicular to the radial fractures. Research addressing the sequencing of radial and concentric of skull fractures in gunshot injuries indicates the radial fractures stem from the point of entry (Viel, 2009; Karger, 2008; Smith, 1987; Leestma, 2009).
The Clark Panel observed extensive fracturing in the autopsy X-rays. The panel report specified there was extensive fragmentation “of the bony structures from the midline of the frontal bone anteriorly to the vicinity of the posterior margin of the parietal bone behind”. The report goes on the state, “throughout this region, many of the bony pieces have been displaced outward; several pieces are missing”. The Clark Panel report indicates the majority of the fracturing and displaced bones fragments are closer to the location they described as the exit wound; this is in direct conflict with scientific research concerning skull fractures resulting from gunshot injuries.
The Kennedy autopsy report stated multiple fracture lines radiated from both the large defect and the smaller defect at the occiput, the longest measuring approximately 19 centimeters. This same fracturing pattern was discussed in the Assassinations Records Review Board deposition of Jerrol Francis Custer, the X-ray technician on call at Bethesda Hospital the night of the Kennedy autopsy. Custer testified the trauma to the head began at the front and moved towards the back of the head (CE 387 16H978; ARRB MD 59:10). Kennedy’s autopsy X-rays have distinct radial fractures propagating from the front of the head, with the preponderance of concentric fractures located at the front of the head. Current research indicates fracturing patterns of this nature correspond with an entry wound located in the front of Kennedy’s head.
Target Movement
When examining the Zapruder film frame by frame, it is readily apparent the President Kennedy’s head moves forward slightly for one frame before his head and shoulders move backward in response to the gunshot wound to the head.
German wound ballistic researcher Bernd Karger, states initial transfer of energy causes the target to move minutely into the force and against the line of fire, prior to target movement with the force of the moving bullet. Karger found greater the transferred energy, the more pronounced the forward movement (Karger, 2008). Wound ballistic researcher Robin Coupland used high-speed photography to confirm and document the forward movement into the line of fire referenced by Karger (Coupland, 2011).
Researchers Karger and Coupland noted the force in a moving bullet is energy of motion, or kinetic energy. Upon impact, the bullet pushes against the head, and initially, as the weight of the head is greater than the weight of the bullet, the head moves against the line of fire. As the projectile slows, more kinetic energy transfers to the target. A overcoming the weight of the head with a sufficient transfer of energy causes the target to move with the continued direction of force of the moving bullet. Application of contemporary wound ballistics research to the movement observed in the Zapruder film indicates a minute forward motion followed by more pronounced rearward movement—consistent with a single shot from the front.
Bullet Fragment Distribution
The distribution of bullet fragment begins near the point of entry and continues in the direction of the bullet trajectory in an ever-widening path as it moves away from the entry wound. A lateral view of the same pattern will reveal a conical shape to the fragment distribution. The apex of the pattern is closest to the entry wound and the wider portion of the fragment cone is closest to the exit wound (Rushing, 2008; Fung, 2008; DiMaio, 1998).
The House Select Committee on Assassinations heard testimony concerning the characteristics of bullet fragment patterns when Larry Sturdivan testified the majority of metallic fragments are typically deposited nearest the entry wound (HSCA 1: 402). Clark Panel Report also stated the majority of fragments were located in the front and top of Kennedy’s head (ARRB MD59:10-11).
Multiple forensic publications indicate X-rays fragment patterns display the majority of fragments near the entry wound. Kennedy’s autopsy X-rays depict the majority of bullet fragments in the front and top of the head, which indicates a frontal shot.
Blood Spatter
Backspatter is blood ejected from the entry wound and travels against the line of fire, back towards the shooter. Although forward and back spatter pattern display some common features, there are also dissimilarities. Studying forward and back spatter patterns created during a singular incident identifies those differences. By differentiating between forward and back spatter in shooting incidents, the identification of the direction of the origin of force is possible (James, 2005).
Scientific journals, books, and research published since the late 1980s indicate the blood observed in the Zapruder film displays the pattern shape of back spatter. It also extends from the wound area a distance characteristic of back spatter, particularly when correlated to blood documented elsewhere on the scene. The timing for the pattern creation and the dissipation rate identifies it as back spatter. In fact, all available information concerning the blood spatter pattern in the Zapruder film corresponds in every measurable manner with back spatter replicated in forensic laboratories and described in peer-reviewed publications since the late 1980s. Consequently, the only possible conclusion is the back spatter in the Zapruder film is genuine. Identifying the blood in the Zapruder film as back spatter signifies a shot from the front of President Kennedy.”~Sherry Fiester CSI
CHAINS OF CUSTODY
“In this article I address the chain of custody for the so-called “magic bullet,” otherwise known as Commission Exhibit 399 (or CE399). According to the Warren Commission, this bullet wounded both President Kennedy and Governor John Connally.
In fact, the chain of custody for this central piece of evidence is non-existent. The true and amazing story about the near-pristine “magic bullet” found at Parkland Hospital shortly after JFK’s assassination has been carefully pieced together by analysts such as Sylvia Meagher in the ’60s and John Hunt in the past few years.
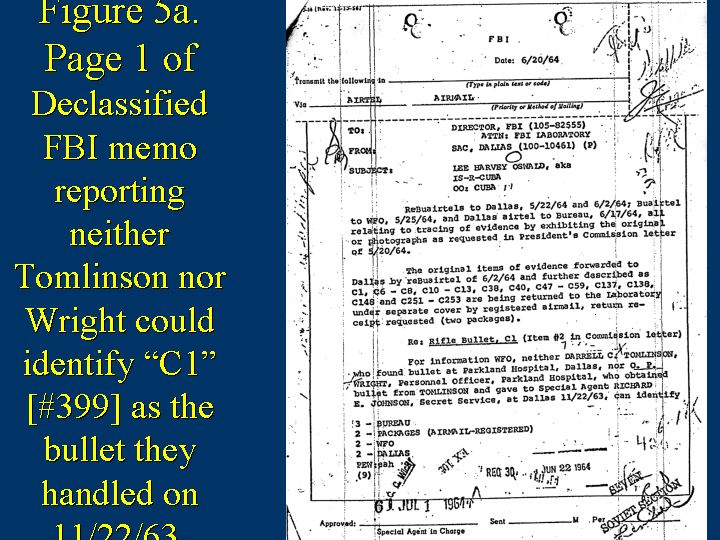
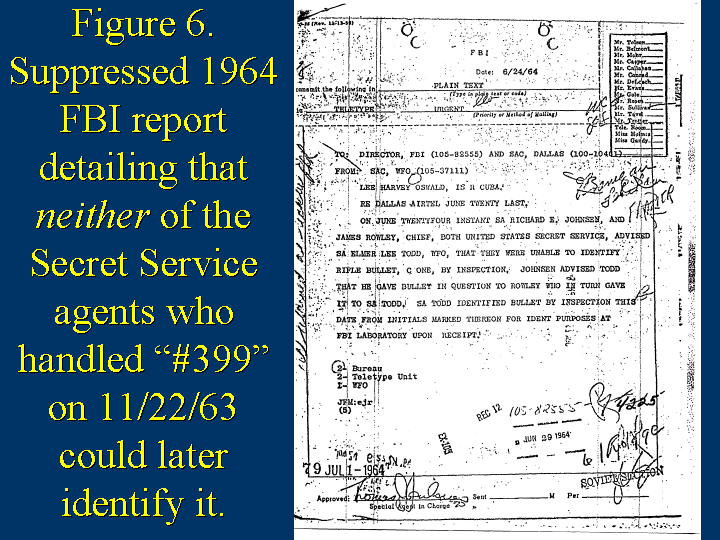
Although Secret Service agent Richard Johnsen received the bullet in Parkland Hospital by about 1:30 p.m., an hour after the assassination, Johnsen’s initials are nowhere on the magic bullet, despite regulations mandating Secret Service agents to initial forensic evidence.
Johnsen handed the bullet to the Secret Service Chief James Rowley at Andrews Air Force Base at about 7:30 p.m., who didn’t initial it either. Neither Johnsen nor Rowley could identify the bullet when shown it later.
___________________________________________
The chief of the Dallas police crime lab, Carl Day, said he initialed all three hulls found on the sixth floor at about 1 pm on the afternoon of November 22.When Day testified on 4/22/64 to the Warren Commission, he had to admit that he did not initial any of them during the time that they were found at the 6th floor of the book depository.
As the hulls are nondescript, initialing them is essential if anyone hopes to recognize such an item again. Detective Richard Sims wrote that after Day took pictures of the hulls, he picked up the “empty hulls”, Day held open an envelope, Sims dropped them in. Sims held onto an unsealed envelope with three hulls in it at 2 pm; at some point, homicide chief Will Fritz was given the envelope by Sims. Fritz later gave the envelope to a sergeant, who eventually brought one hull back to Fritz and the other two hulls back to Day.
Day admitted during his Warren Commission testimony that he only initialed the two hulls in the unsealed envelope when he got it back at 10 that night. Day passed the shells on to FBI agent Vince Drain in the early morning, and I am similarly unaware of any record of Drain initialing any of these materials before he passed them on to firearms expert Robert Frazier at the FBI lab. Frazier’s testimony doesn’t mention anything about these shells being initialed by either of these men.
These hulls should have been excluded based on the failure to have a reliable chain of custody.”
~Bill Simpich

Darrel Tomlinsen told Josiah Thompson in an interview that this is what the bullet looked like that he had found on the stretcher at Parkland. It looks like a 30-30, and is certainly not CE399.
http://history-matters.com/essays/frameup/EvenMoreMagical/EvenMoreMagical.htmThe Parkland Bullet & Broken Chain of Custody to CE399

Within an hour after the assassination, Johnsen was given the bullet by Parkland hospital security director O.P. Wright, after orderly Darrell Tomlinson found it by a stretcher. Like Johnsen and Rowley, neither Wright nor Tomlinson could identify the bullet.
_______________________________________________________________The first 4 links in the chain of custody of the bullet found a Parkland are unable to identify it as CE399.
They are:1. Orderly Darrell Tomlinson >>
2. Parkland hospital security director O.P. Wright >>
3. SS Agent Richard Johnsen >>
4. Agent Rowley (Secret Service Chief).A break in the chain of custody at this proximate point proves that the bullet of record, CE399 is NOT the bullet found at parkland, and therefor CE399 is a planted bullet by the highest authorities themselves.
Let me remind you once again: A memorandum from the FBI office in Dallas on June 20th to J. Edgar Hoover contains the statement, “neither DARRELL C. TOMLINSON [sic], who found bullet at Parkland Hospital, Dallas, nor O. P. WRIGHT, Personnel Officer, Parkland Hospital, who obtained bullet from TOMLINSON and gave to Special Service, at Dallas 11/22/63, can identify bullet”
http://www.maryferrell.org/showDoc.html?docId=59607#relPageId=29
http://www.maryferrell.org/showDoc.html?docId=59607#relPageId=86Warren Commission Testimony vol. VI
TESTIMONY OF DARRELL C. TOMLINSON
The testimony of Darrell C. Tomlinson was taken on March 20, 1964, at Parkland Memorial Hospital, Dallas, Tex., by Mr. Arlen Specter, assistant counsel of the President’s Commission
http://jfklancer.com/docs.maps/tomlinson.html
However, at the time Tomlinson was questioned by Specter, he had not seen CE399. When Tomlinson finally did see CE399, he said that it was not the bullet he found at Parkland.The Parkland Bullet is a distinct and different bullet from CE399.

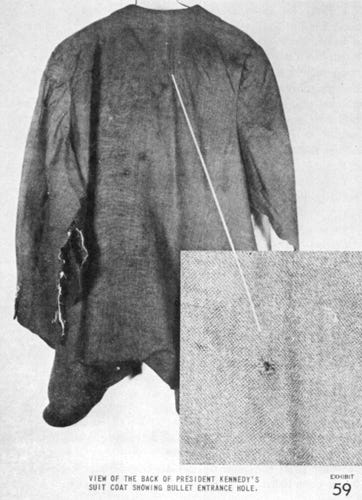
The hole in the jacket was 5.5 inches below the upper margin of the jacket collar, and the hole in the shirt, 5 3/4 below the upper margin of the shirt collar [7 HSCA 83] about where witnesses said the back wound was – well below the base of the neck.
Mr. KLEIN: And with respect to the wounds to the President’s back, what did the panel learn from that clothing?
Dr. BADEN: In the jacket and the underlying shirt there is a perforation of the fabric that corresponds directly with the location of the perforation of the skin of the right upper back that, the panel concluded, was an entrance gunshot perforation that entered the back of the President.
This is correspondingly seen in the shirt beneath.
[1 HSCA 196: http://www.history-matters.com/archive/jfk/hsca/reportvols/vol1/pdf/HSCA_Vol1_0907_5_Baden.pdf%5D
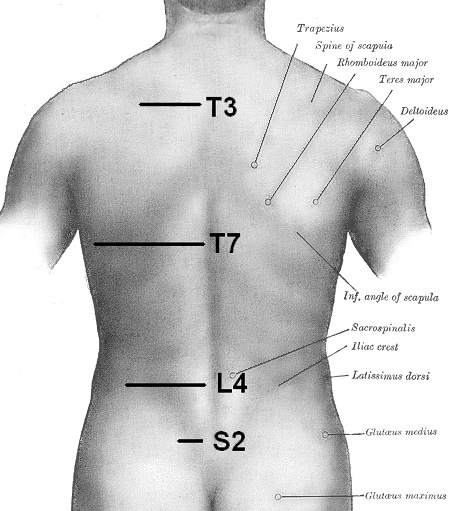
This should make it perfectly clear where T-3 is located:
> Exactly where Kennedy’s back wound is in Boswell’s autopsy facesheet.
> Exactly where Kennedy’s back wound is in that photograph.
> Exactly where Kennedy’s back wound is in his shirt.
> Exactly where Kennedy’s back wound is in his coat.
> Exactly where Kennedy’s back wound is in Burkley’s autopsy report.
> Exactly where Kennedy’s back wound is as told by SS Agent Sibert.On 11-22-63, at 3:16 PM CST, barely two hours after JFK was pronounced dead, Perry appeared with Kemp Clark, MD, the professor of neurosurgery who had pronounced JFK dead.
A newsman asked Perry: “Where was the entrance wound?”
Perry: “There was an entrance wound in the neck…”
Question: Which way was the bullet coming on the neck wound? At him?”
Perry: “It appeared to be coming at him.”…
Question: “Doctor, describe the entrance wound. You think from the front in the throat?”
Perry: “The wound appeared to be an entrance wound in the front of the throat; yes, that is correct. The exit wound, I don’t know. It could have been the head or there could have been a second wound of the head. There was not time to determine this at the particular instant.”[66] (emphasis added)
Read the how Perry was badgered into changing this clear and straightforward opinion by Arlen Specter, and the PR Machine:
http://www.history-matters.com/essays/jfkmed/How5Investigations/How5InvestigationsGotItWrong_1b.htm
Boswell Sent To Garrison Trial To Shut Up Dr Finck
Q. Very early on in your deposition today, you made reference to Mr. Eardley from the Justice Department asking you to go to New Orleans; is that correct?
A. Mm-hmm.
Q. What did he say to you about the reason he wanted you to go to New Orleans?
A. He was really upset. He says, “J, we got to get somebody in New Orleans quick. Pierre is testifying, and he’s really lousing everything up.” And I called Jim to see if he didn’t want to go, and he was having–his mother-in-law was ill, and he couldn’t go. So they put me on a plane that day and took me to New Orleans, and that was one of the most interesting adventures of my life. I met–do you want to hear all of this?
Q. Yes, please.
A. Carl Eardley sent me to a hotel, and I went into the hotel and registered. I was already registered. I got up to my room, and there was a note on my bedside table telling me to meet somebody at a certain place at a certain time. And this was a scary place. This was down around the wharfs, and the federal attorney’s office was in a big warehouse down there. And that’s–I met somebody on the street. He took me in there, and then they told me what was going on. They showed me the transcript of Pierre’s testimony for the past couple of days, and I spent all night reviewing that testimony. And it was this bit about the general. Jim said, “Who’s in charge here?” And when they asked Pierre in court who supervised and ran the autopsy, he says, “Some Army general.” And so that is why–and I never appeared. I spent two days down there and then came home, never appeared in court. And the government won their case.
Q. Actually, the government was the district attorney. So my next question for you actually was: What was the United States Department of Justice doing in relationship to a case between the district attorney of New Orleans and a resident of New Orleans?
A. Well, they–I went over and met somebody, some lawyer in another firm that night, and I don’t know who he was representing. But, obviously, the federal attorney was on the side of Clay Shaw against the district attorney.
Q. Do you remember the name of that federal attorney?
A. No. I have no idea.
Q. Was it Harry Connick?
A. It could very well have been. That name sounds–of course, Connick is not an uncommon name. It could have been.
Q. Do you recall meeting with an attorney named Wegman?
A. No.
Q. Or Dymond?
A. Thirty years ago, no, I can’t remember that.
Q. What did the government attorney say to you? Did he help prepare potential testimony for you?
A. They were getting ready to. I guess it all depended on what Pierre did that next day or something. I don’t know. All I know is that they- -he was answering in very strange ways their questions, and, yes, they sent me down and talked to me and tried to get me to agree that he was very strange and that I could do a better job or something.
Q. Did you ever talk to Dr. Finck about his testimony?
A. No.
Q. Did you ever talk to him at all after that point?
A. Oh, yes, many times. Pierre’s wife was there with him, and he was staying in the same hotel I was. And so we met just by chance at breakfast the day after I arrived. And we didn’t discuss why I was there. I’m sure he asked me, and I don’t know what I told him. But, anyway, we have met on a number of occasions since then. His daughter is in this country, and she was going to school in Missouri for several years. And I used to–they’d stop by here and visit with us as they were on their way. We were very good friends.
Q. Do you have any idea why he was answering the questions the way he was in the Clay Shaw trial?
A. Well, you’ll know when you meet him, if and when you meet him. He is a very strange–but a sharp guy. He was a good pathologist, a hard worker. He was devoted to the United States and to the Army despite the fact that he was going back home. But he’s a strange guy. I knew that long before we invited him over to help us on this autopsy. He’s just a strange fellow.
Q. Do you recall who paid for your trip to go to New Orleans?
A. I would assume that the Justice Department provided my plane tickets and my hotel bill.
Q. Other than for this experience in New Orleans, were you contacted at any other point by any representative of the U.S. Government to provide assistance for the government in regard to the Kennedy autopsy?
A. No. But aside from that, Carl Eardley called me when King was assassinated and said, “J, we got a problem down in Memphis. They’re alleging that we’re letting the Reverend die.” And then he called me back and said, “He died. Would you go down there and supervise the autopsy?” And I said I’m the last–by this time, it had been several years, and we’d had an awful lot of stuff about the autopsy. And so I said, “I’m the last one you want to go down.” And I gave him the name of the guy who was at that time the neuropathologist–I knewwhat they were going to find because he had been shot in the neck and the spinal cord was severed. And I gave him the name of the neuropathologist at the AFIP, and he called him and got him to go.
That’s the only other incident relative to that.Page 213 forward ARRB Deposition of Boswell
http://mcadams.posc.mu.edu/russ/testimony/boswella.htm
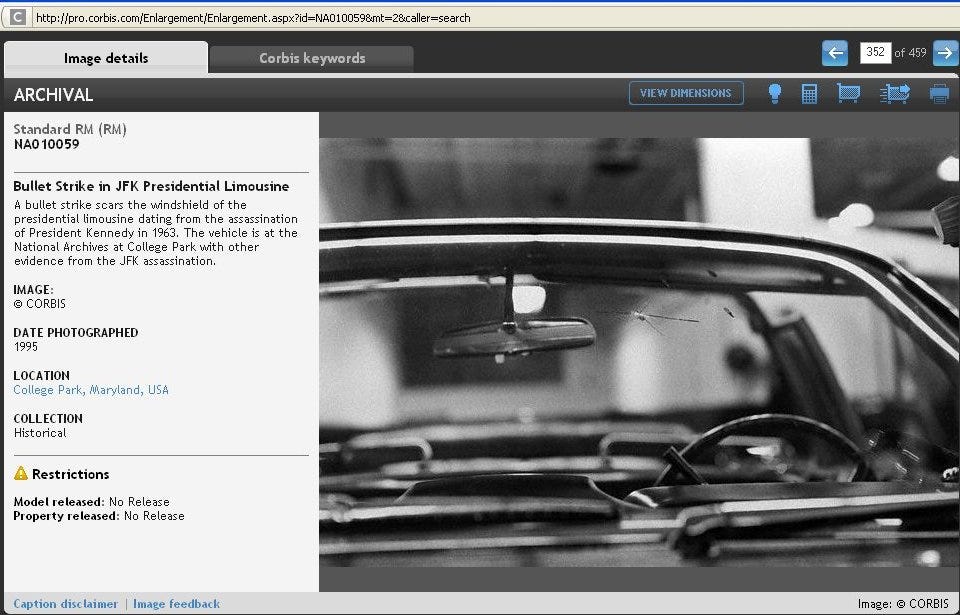
Additional damage to the windshield and/or the rear-view mirror of SS100X
There is so much more to this issue that I want to publish here. So I will also be uploading more info in the comments section.
\\][//
I visited the Sixth Floor Museum and fell apart. Do you know Dallas PL has this collection? https://dallaslibrary2.org/dallashistory/kennedy.php
I worked in Louisiana where this remains a much discussed. Then I worked in Tampa where JFK had been before Dallas. James Ellroy brought it all back. Minsk. So much. Oswald's Tale.